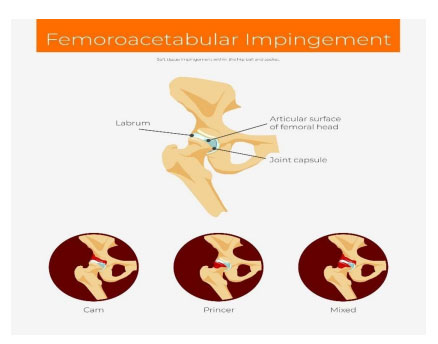
Femoroacetabular impingement (FAI) is caused by irregular bone growths (bone spurs) that are not able to fit properly along one or both bones that form the hip joint. When these irregular bone growths rub against each other during movement, damage to the cartilage and labrum occurs, causing pain and decreased physical activity. Overtime, this damage may lead to degeneration and development of hip osteoporosis (OA). Though the cause of FAI is unknown, studies have found that athletes with a history of high impact sports (soccer, basketball, ice hockey, etc.) and adolescents have a higher
prevalence of FAI than non-athletes. FAI may begin in adolescence and continue through adulthood.
Patients may complain of hip stiffness, front and front-lateral hip pain that travels to the groin and radiates down the front of the thigh, and increased pain during activities that require bending at the hip and/or internal rotation. Sitting, squatting, and driving can aggravate the symptoms. If patients complain of clicking of the hip or stiffness, then they may have a labral tear or chondral damage. A tight psoas tendon or iliotibial (IT) band may be evident during physical assessment. A change in gait patterns, decrease in hip range of motion, and lower muscle strength may be noticeable. Children may have difficulty describing pain and may limp after activity.
These patients will be assessed by their primary care physician or general practitioner. Diagnosis of femoracetabular impingement (FAI) is based on the results of a hip X-ray to assess acetabular or femoral anatomy and to identify OA of the hip, a magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) to show labral and articular cartilage damage, and a 3D assessment of bone deformity and pressure of impingement cysts. These results will be used to help with surgical planning.
The treatment plan depends on the severity of the pain. If pain is tolerable, meaning there is a reduction in hip pain, symptoms improve, and disability declines by a focus on activity modification, movement pattern retraining, muscle strengthening and pain management, surgery will not be necessary. However, if the pain is unbearable, then surgical treatment may be needed. These patients will be referred for an orthopedic consult for surgery. The goal is to correct anatomical abnormalities of the hip joint, repair cartilage damage, decrease degeneration of the joint, and prevent hip osteoporosis (OA).
If you or someone that you know is experiencing any of the symptoms described above, please consult with your primary care physician (PCP) or general practitioner (GP) as soon as possible.
References
M_Denis. (2020). [Diagram]. Femoroacetabular impingement cheme anatomy poster.
https://www.shutterstock.com/image-vector/femoroacetabular-impingement-cheme-anatomy-poster-1746776624.
OrthoInfo. (2020). Femoroacetabular impingement. https://orthoinfo.aaos.org/en/diseases–conditions/femoroacetabular-impingement/.
Pun, S., Kumar, D., & Lane, N. E. (2015). Femoroacetabular impingement. Arthritis & rheumatology (Hoboken, N.J.), 67(1), 17–27. https://doi.org/10.1002/art.38887.