Shoulder Anatomy
The shoulder is formed where the humerus, collar bone (clavicle), and scapula join. The rotator cuff holds the humerus in place. The muscles that form the shoulder are the supraspinatus, infraspinatus, tres minor, subscapularis, and deltoid. There are four rotator cuff tendons and two biceps tendons that make up the shoulder. These tendons connect the deep layers of the muscles to the scapula and humerus and provide support to the glenohumeral joint. The supraspinatus tendon is the most affected tendon due to overuse and trauma. The supraspinatus muscle is responsible for lifting the arms out to the side. An injury to this muscle can result in a possible rotator cuff tear or tears. Overuse can lead to shoulder (subacromial) impingement.
Shoulder Dislocation
Shoulder dislocations are caused by falling accidentally or while playing sports (football, basketball, baseball, soccer, etc.). Patients who have dislocated their shoulder report hearing and feeling a pop in their shoulder when the head of the humerus comes out of its socket, the glenoid.The affected shoulder will be visibly out of place. Patients will experience increased pain, increased shoulder weakness, decreased shoulder mobility, swelling, bruising, muscle spasms, numbness, tingling in the arm, back, and fingers. If you or someone else has dislocated a shoulder, please do not move the arm.Go directly to the ER or call 911. Do not try to reset the shoulder on your own. Doing so may cause severe damage to the nerves, blood vessels, muscles, and ligaments. Apply ice packs to the shoulder to help reduce swelling and pain. NSAIDS, such as Advil and Aleve, or Tylenol will be helpful for pain relief.
While in the ER, a shoulder X-ray and a 2-view shoulder MRI/CT with contrast will show damaged ligaments torn by the shoulder dislocation. The most important treatment for acute shoulder dislocation is immediate reduction of the glenohumeral joint. The glenohumeral joint is the most dislocated joint in the body. Shoulder dislocations can occur anteriorly (front), posteriorly (back), inferiorly (towards the armpit), and anteriorly-superiorly (front and upwards). A shoulder dislocation that is anterior-superior will occuras a result of a complete rotator cuff tear when the ligament is no longer attached or from an unsuccessful shoulder surgery. Patients with a previous shoulder dislocation are more likely to dislocate their shoulder again because the tissue does not properly heal or because the tissue becomes too laxed.
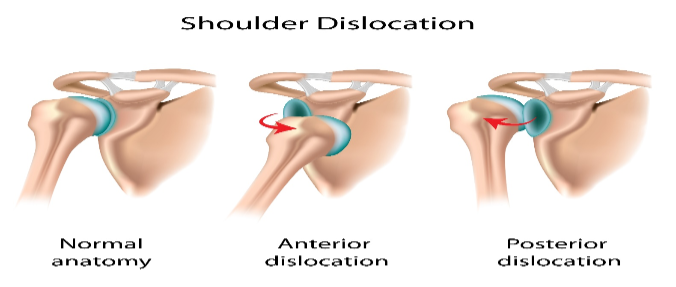
The shoulder stability is maintained by the glenohumeral ligaments, joint capsule, and rotator cuff muscle. The inferior glenohumeral ligament is the most important and the most injured during an anterior shoulder dislocation. In this type of dislocation, the ligaments are torn off the bony attachments, and there may be possible fractures to the glenoid or humerus. Rotator cuff tears can also lead to shoulder instability, especially large rotator cuff tears. Shoulder instability can also be caused by a damaged nerve that controls the shoulder muscles.
The recovery time for a dislocated shoulder takes several weeks to several months depending on the severity and need for surgery. Please follow the directions of your orthopedic surgeon and physical therapist for a healthy recovery.
References
Alina Medical Media. (2019). Dislocated Shoulder. [Diagram]. Retrieved from https://www.shutterstock.com/image-illustration/dislocated-shoulder-121783261?src=library
Cothran, V. (2018). Shoulder Dislocation. Retrieved from https://emedicine.medscape.com/article/93323-overview
NIH. (2019). Dislocated Shoulder. Retrieved from https://medlineplus.gov/dislocatedshoulder.html