Sternal fractures result from blunt force trauma to the chest. Before the passage of the seatbelt laws, sternal fractures occurred in approximately 3% of MVAs. Of course, the percentage has declined over time. Sternal fractures can be caused by a variety of ways: direct impact sports, falls, car accidents, assault, spontaneous, stress fractures, and in women with osteoporosis and kyphosis of the thoracic spine. Long-term steroid use and CPR can also cause rib and sternal fractures. Sternal fractures appear in the midbody and transverse area of the sternum (breastbone). Manubrium fractures are the most common.
When this fractures occur, patients will complain of localized sternal pain, or pain may cover the entire chest. If anyone experiences this type of pain, it is especially important to call 911 and go directly to the nearest ER in order to rule out a myocardial infarction (heart attack). This type of injury has a mortality rate of less than 1% unlike chest injuries like cardiac contusions, aortic rupture, pulmonary contusion, and thoracic spine compression fractures. Difficulty breathing is present in 15% to 20% of the patients, which may be caused by a cardiopulmonary contusion. Elderly patients with chest wall fracture may be placed on observation at the hospital because they have increased risk for respiratory compromise and atelectasis. Once in the ER, cardiac work-up to rule out a heart attack will begin. EKGs will be repeated every 6 hours. However, if the EKG results are normal, no further work-up is required. Anterior, posterior, and lateral view X-rays will be performed if there is suspicion of sternal
fracture. An anterior-posterior view X-ray can be helpful in detecting other injuries: rib fractures, pulmonary contusion, hemothorax, and pneumothorax. A chest CT is the most common image study to assess the degree of sternal displacement and other chest injuries.
Surgery fixation is not necessary for patients with sternal fractures. Treatment for sternal fractures can be performed as an outpatient procedure unless other injuries are associated with the injury. Pain management follow-up may be necessary for medication. Patients do tend to recover quickly (several weeks’ time) from isolated sternal fractures.
The fractures in children should cause suspicion of abuse. Please follow-up with a pediatrician, family physician, or nearest ER as soon as possible. If you suspect that the child may be in danger, please all the police and child protective services.

References
Felten, S. (2017). Sternal Fracture Differential Diagnoses. Retrieved from
https://emedicine.medscape.com/article/826169-differential
Marchal, D. (2020). [Illustration]. Digital medical illustration depicting a fracture of the breastbone (sternum). Anterior (front) view. 3D rendering. Retrieved form https://www.shutterstock.com/image-illustration/digital-medical-illustration-depicting-fracture-breast-1399874504
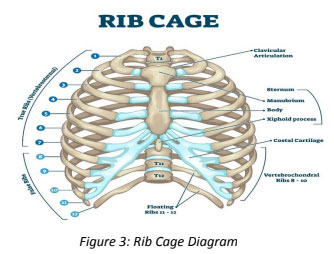
VectorMine. (2020). [Illustration Diagram]. Rib cage anatomy, labeled vector illustration diagram.
Medical human chest skeletal bone structure model. Numbered ribs, sternum, cartilage parts and clavicular articulation. Health care education. Retrieved from
https://www.shutterstock.com/image-vector/rib-cage-anatomy-labeled-vector-illustration-1650017491